














































































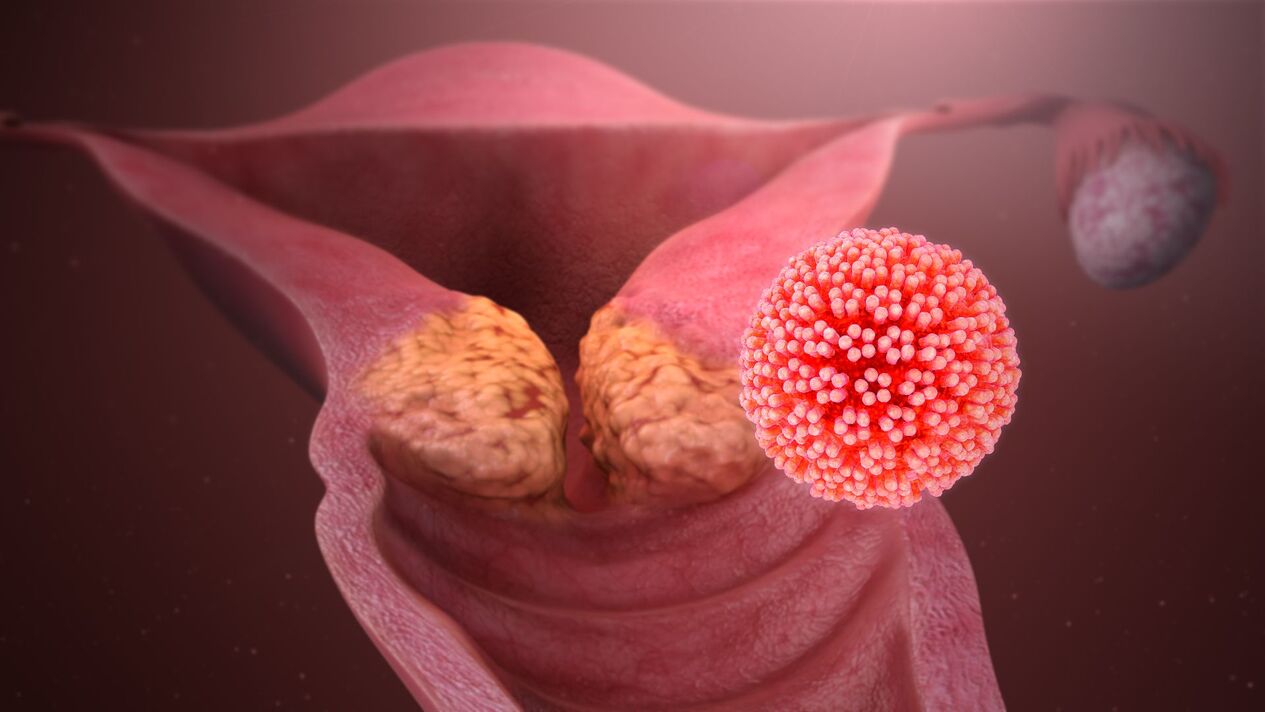
Human papillomavirus (HPV) is an extremely common sexually transmitted infection worldwide.
The peculiarity of this infection is that it may not appear for many years, but eventually lead to the development of benign diseases (papilloma) or malignant (cervical cancer) of the genitals.
Types of human papillomavirus
More than 100 types of HPV are known. Species are specific "subspecies" of a virus that differ from one another. Species are determined by the numbers assigned to them when they were discovered.
The high oncogenic risk group consists of 14 types: 16, 18, 31, 33, 35, 39, 45, 51, 52, 56, 58, 59, 66, 68 (these types are associated with the development of cervical cancer).
In addition, low oncogenic risk species (mainly 6 and 11) are known. They lead to the formation of anogenital warts (genital warts, papillomas). Papillomas are located in the mucosa of the vulva, vagina, perianal region, on the skin of the genitals. They almost never become malignant, but lead to significant cosmetic defects in the genital area. Warts on other parts of the body (hands, feet, face) can also be caused by these types of viruses or can have a different origin. In the following articles, we will discuss separately the types of HPV "high risk" and "low risk".
Human papillomavirus infection
The virus is transmitted mainly through sexual contact. Almost all women become infected with HPV sooner or later: up to 90% of sexually active women will experience this infection in their lifetime.
But there is good news: the majority of those infected (about 90%) will recover from HPV without any medical intervention within two years.
This is the normal course of the HPV-induced infectious process in the human body. This time is enough for the human immune system to completely rid itself of the virus. In such a situation, HPV will not cause any harm to the body.That is to say, if HPV was discovered some time ago, and now it is not, this is absolutely normal!
It should be borne in mind that the immune system works in different people at "different speeds". In this regard, the rate of HPV removal may be different for sexual partners. Therefore, a situation is possible when HPV is detected in one of the partners, and not in the other.
Most people become infected with HPV as soon as they become sexually active and many will never know they are infected with HPV. Permanent immunity does not develop after infection, so it is possible to re-infect yourself with the same virus that has already been encountered, as well as with other types of virus.
High-risk HPV is dangerous because it can lead to the development of cervical cancer and some other types of cancer. High-risk HPV does not cause other problems.
HPV does not lead to the development of inflammation in the mucosa of the vagina / cervix, menstrual irregularities or infertility.
HPV does not affect the ability to conceive and perform a pregnancy.
A baby with "high-risk" HPV is not transmitted during pregnancy and childbirth.
Diagnosis of human papillomavirus
It is practically useless to get an HPV test for high oncogenic risk before the age of 25 (except for those women who start having sex early (before the age of 18)), as at this time it is very likely to detect a virus that will soonleave the body alone.
After 25-30 years, it makes sense to do an analysis:
- together with a cytological analysis (PAP - test). If there are changes in the PAP test, and HPV "high risk", then this situation requires special attention;
- The long-term persistence of "high-risk" HPV in the absence of cytological changes also requires attention. Recently, the sensitivity of the HPV test in the prevention of cervical cancer has been shown to be higher than the sensitivity of cytology, and therefore the sole determination of HPV (without cytology) has been adopted as an independent prevention studyof cervical cancer. in the United States. However, in our country an annual cytological examination is recommended, so it seems reasonable to combine these two studies;
- after treatment of dysplasia / precancerous / cervical cancer (absence of HPV in post-treatment analysis almost always indicates successful treatment).
For the study, it is necessary to take a stain from the cervical canal (it is possible to study the material from the vagina, however, as part of the examination, it is recommended to take the material from the cervix).
The analysis should be given:
- 1 time per year (if "high-risk" HPV is previously detected and the test is given in conjunction with a cytological examination);
- 1 time in 5 years if previous analysis was negative.
It is almost never necessary to have a low-risk oncogenic HPV test. If there are no papillomas, then this analysis makes no sense in principle (virus transmission is possible, there is no treatment for the virus, so it is not known what to do next with the test result).
If there are papillomas, then:
- most commonly caused by HPV;
- they should be deleted regardless of whether or not we find types 6/11;
- if we get a stain, then directly from the papillomas themselves, and not from the vagina / cervix.
There are tests to detect different types of HPV. If you do a periodic HPV test, pay attention to what specific types are included in the test. Some labs do research only for types 16 and 18, others - for all types together. It is also possible to do a test that will identify all 14 types of "high risk" virus in a quantitative format. Quantitative characteristics are important in predicting the likelihood of developing precancerous and cervical cancer. These tests should be used in the context of cervical cancer prevention and not as an independent test. Analysis for HPV without cytological results (PAP test) most often does not allow any conclusion to be drawn about the patient's state of health.
There is no such analysis that will determine whether the virus in a given patient will "leave" or not.
Treatment of human papillomavirus
There is no medical treatment for HPV. There are treatments for HPV-induced conditions (papilloma, dysplasia, precancerous, cervical cancer).
This treatment should be performed using surgical methods (cryocoagulation, laser, radiothics).
No "immunostimulants" are related to the treatment of HPV and should not be used. None of the widely known drugs in our country has passed adequate tests that would show their effectiveness and safety. None of the protocols / standards / recommendations include these drugs.
The presence or absence of "erosion" of the cervix does not affect HPV treatment tactics. You can read more about those situations when it is necessary to address erosion in the article "Erosion or not erosion? ".
If the patient has no complaints, and there are no papillomas / changes in the cervix during the colposcopy and according to the PAP test, no medical procedures are needed.
It is only necessary to retake the test once a year and monitor the condition of the cervix (annual PAP test, colposcopy). In most patients, the virus will "leave" the body on its own. If left untreated, it is not at all necessary to lead to the development of cervical cancer, but control is needed.
Treatment of sexual partners is not required (unless both partners have genital papillomas).
Prevention of human papillomavirus infection
Vaccines have been developed to protect against HPV types 16 and 18 (one of the vaccines also protects against types 6 and 11). HPV types 16 and 18 are responsible for 70% of cervical cancer cases, which is why protection against them is so important. Routine vaccination is used in 45 countries around the world.
Condom (does not offer 100% protection).
The only method that provides 100% protection is abstinence from sexual intercourse. By no means am I campaigning for it, I're just giving food for thought.